“Come look at his knees,” a concerned parent asked me.
The toddler climbed off the couch and ran, no, barreled towards me.
“Look! When he stands, his knees are touching! What’s wrong with his legs?”
“He’s 2-years-old, right?” I asked.
“Yes,” said the mom.
“Nothing, this is typical knee alignment for his age. Let me explain…”
Parents are most concerned about bowlegs (genu varum) and knock- knees (genu valgum) in their children. As early intervention providers, we are in a unique position to educate parents and caregivers about the normal development of hip and knee alignment, as well as assist families in deciding when it is appropriate to seek the expertise of an Orthopedist.

As a child grows, from infancy to childhood, the alignment of the knee also changes. At birth, newborns are bowlegged (genu varum). The infant’s legs slowly straighten and between 12-24 months old, the legs reach a neutral alignment. It has been suggested that the alignment of the knees improves as weight bearing increases during standing activities between 12-24 months. Knock-knees (genu valgum) reach its peak between the ages of 2 and 4 years-old and then gradually decreases. The final knee position differs depending upon the gender of the child. Sixteen-year-old females tend to have slight knock-knees as their pelvises are wider. Sixteen-year-old males tend to have slight bowlegs as their pelvises are narrower.
It makes sense then, that the reason the greatest number of referrals to Orthopedists of children between the ages of 2 and 4 years-old are for concerns of knee alignment. That’s when knock-knees reaches its peak! The change from straight (or neutral) legs to knock-knees can be disconcerting for parent.
There is good news! Eighty percent (80%) of children with bowlegs before age 2 years-old and knock-knees before age 6 years-old, will improve knee alignment spontaneously. There are various opinions about when or if knock-knees and bowlegs warrant treatment. Research has found that twister cables and other conservative, non-operative treatments are unsuccessful. Evidence suggests that therapists should measure hip range of motion every 6 to 12 months to document femoral anteversion (inward rotation of the femur; resultant knee turning inward).
Children should be referred to an Orthopedist if they have:
– Excessive knock-knees or bow legs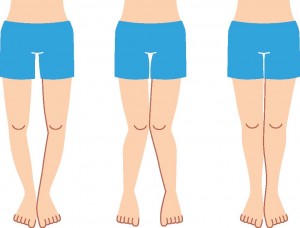
– One leg is more or less knock-kneed or bow legged than the other (asymmetrical)
– Knock-knees or bowlegs progressively increase
– Pain with putting weight on their legs
– One leg longer or shorter than the other leg
– Knock-knees or bowlegs persist beyond 7-8 years-old
– Position of the knees create significant cosmetic and functional disability
How have you addressed this concern with the families you work with?
References
Cheng JCY, Chan PS, Chiang SC, HUI PW. Angular and rotation and profile of the lower limb in 2,630 Chinese children. Journal Of Pediatric Orthopedics. 1991; 11:154-161.
Heath CH, Staheli LT. Normal limits of knee angle in white children – Genu varum and genu valgum. Journal of Pediatric Orthopedics. 1993; 13:259-262.
Staheli LT. Fundamentals of pediatric orthopedics. 4th ed. Philadelphia: Wolters Kluwer, Lippincott Williams & Wilkins; 2008.
Campbell S, Vander Linden DW, Palisano RJ. Physical Therapy for Children. 3rd ed. Missouri: Saunders Elsevier; 2006.
Effgen S. Meeting the physical therapy needs of children. 2nd ed. Philadelphia: FA Davis Company; 2013
Sass P, Hassan G. Lower Extremity Abnormalities in Children. American Family Physician. 2003; 68(3):461-468.
Ganger R. Lower Limb Development. www.scribd.com/doc/55666675/Lower-Limb-Development-Ganger. Published 2011. Accessed August 2, 2014.
Thanks for this great information, Kim. My oldest daughter had femoral anteversion and I clearly remember my worries. Your list of when to seek an orthopedist’s opinion is most helpful. And…I’m happy to report that my daughter had good resolution and became a masterful soccer player. 🙂